University of Iowa researchers are working to connect migraine patients with the treatments that will actually work for them.
Story: Christina Hernandez Sherwood
Photography and illustration: UI Health Care Marketing and Communications
Published: April 30, 2026
For most of her life, Andrew Russo's mother kept the curtains drawn in the family home.
"She just never liked the light," says Russo, PhD, a professor in the Department of Molecular Physiology and Biophysics at the University of Iowa Carver College of Medicine. Her migraine disorder went undiagnosed for years — as it did for millions of others. "From a scientific perspective, it wasn't recognized as a real biochemical disorder."
Russo has spent the past 40 years trying to change that. His research on a protein linked to migraine helped lead to the first-ever FDA-approved migraine prevention drug, erenumab (Aimovig), in 2018. He also holds two patents related to eptinezumab (Vyepti), a second prevention therapy approved in 2020. Today, eight related treatments are on the market — and two of Russo's three daughters are among the patients who have benefited.
"I feel like I backed the right horse," he says.
A disorder hiding in plain sight
Migraine is one of the most common — and most misunderstood — conditions in the world. Headache disorders affect more than 4 billion people globally, and roughly one-third experience migraine. Beyond intense head pain, the condition can cause nausea, vomiting, and extreme sensitivity to light and sound. The World Health Organization places severe migraine in the same disability category as quadriplegia and terminal cancer.
Despite this, migraine was long dismissed — particularly in women — as something less than a legitimate medical condition.
"Think of the fainting Victorian lady unable to deal with life," Russo says.
Today's treatments help many patients, but finding the right one can take months or even years of trial and error.
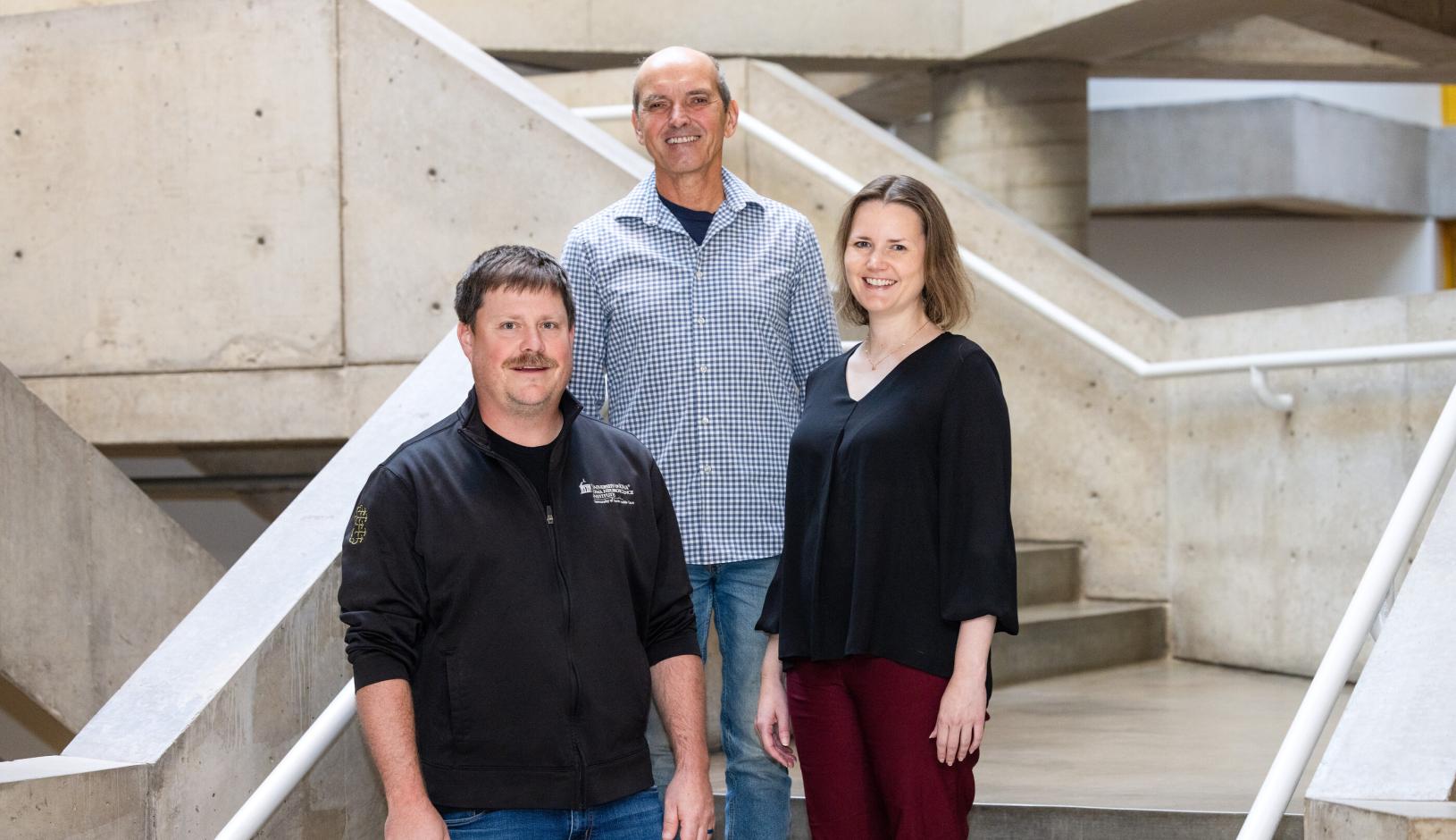
Iowa Neuroscience Institute researchers (from left) Levi Sowers, Andrew Russo, and Rainbo Hultman are integrating their research specialties with the goal of establishing new paradigms in migraine treatment.
A team takes shape
Now Russo is collaborating with two colleagues whose expertise can take migraine research in new directions. Rainbo Hultman, PhD, an assistant professor in the Department of Molecular Physiology and Biophysics, studies how multiple brain regions work together. Levi Sowers, PhD, an assistant professor in the Stead Family Department of Pediatrics and its Division of Child Neurology, focuses on post-traumatic headache — a migraine-like condition triggered by brain injury that doesn't respond well to existing migraine medications.
Like Russo, both have personal reasons to care.
Migraine has run through Hultman's family for generations. Her grandmother's sister, she says, "missed out on much of her life with frequent debilitating migraine attacks over decades of her life." Watching family members struggle helped her recognize migraine as a whole-brain problem.
"People are having symptoms of nausea and sensitivity to different sensory modalities. They're having pain and emotional changes. They're yawning or can't find their words," she says. "It was clear to me that this is a systems neuroscience problem."
Hultman had followed Russo's research from afar during her graduate training at Duke University. His findings were groundbreaking, but not without skeptics — even the idea of studying headache in mice was once considered far-fetched.
"There was a lot of doubt about whether animals actually get headaches," Russo says, "which is extremely ethnocentric of us to think evolution has favored humans with headache."
"Anytime there is something that exciting and impressive, I know it comes with a lot of haters along the way," Hultman says. "I'm so thankful he stuck with it."
Sowers trained in Russo's lab, where the two studied another protein linked to headache, PACAP, and developed a PACAP-targeting drug now in clinical trials.
Together, the three researchers converged around a shared question: why are some people — or mice — more resistant to migraine triggers than others? Sowers describes it simply: they "came together through this idea of headache resilience."
"It's very unique to bring three people with the expertise we have together to do what we're doing," he says.
Inside the migraine brain
To understand resilience, the team is building an unprecedented picture of what happens in the brain during a migraine attack. Russo will study gene activity across different brain regions in mice that respond to migraine-inducing proteins versus those that don't. Hultman will measure electrical brain signals to identify patterns linked to resilience. Sowers will help translate findings from mice to humans using advanced brain imaging.
"It's amazing what [Hultman] can do with those electrodes," Russo says. "[Sowers] has the expertise to use advanced techniques like fMRI in mice. I, and other colleagues, tried doing fMRI in mice years ago. At that time, the tools were not there."
Those tools are now available through the Iowa Neuroscience Institute, which has funded the group's collaboration through a grant from the Roy J. Carver Charitable Trust.
"Iowa and the Carver Trust have made a real commitment to neuroscience research," Russo says. "It has helped us make advances, and it's helping us now move forward, which we wouldn't be able to do with one lab on its own."
Rainbo Hultman holds a multi-site recording electrode used in lab mice to measure neural signals related to migraine and migraine resistance.
The right treatment, sooner
The team's goal isn't necessarily to develop new drugs — though that's possible. Their main aim is to match patients with the treatments most likely to work for them.
"We're collecting data on how existing medications impact different brain network activities," Hultman says. "Within a couple of years, we could have some ability to predict the current therapeutics matching with specific brain network activities."
In practice, that could mean testing a patient's brain activity to determine their "type" of migraine — and then directing them toward the most effective option, whether that's a targeted drug, an injectable antibody therapy, or a device that stimulates the nervous system.
The urgency is real. The more frequently someone experiences migraine, the more likely the condition is to become chronic — especially when it begins in childhood. Early, effective treatment can change that trajectory.
"There is this great need for precision medicine where you can intervene early and get the right answer for that specific patient right away," Hultman says.